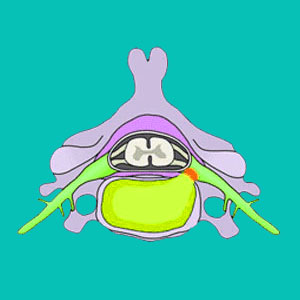
A foraminal herniated disc may also be known by several other terminologies, including a foraminal disc bulge or foraminal disc protrusion. These herniations are similar to paramedial herniated discs, in that they bulge off center to the left or to the right. However, in the case of foraminal bulges, the disc blocks off some or all of the neuroforaminal opening, through which the spinal nerves exit at the affected level. This can occasionally cause a pinched nerve to occur, when considerable force is enacted against the neurological structure.
This dialog will concentrate on discussing how foraminal herniations can affect nerve tissue and why so many are misdiagnosed as the actual source of back or neck pain.
What is a Foraminal Herniated Disc?
The neuroforamen is a space on either side of the vertebrae through which nerve roots pass out of the central canal at every spinal level. There are left and right foramen at each level and nerve roots exit on both sides of the vertebral column. Neuroforamen can be partially or completely blocked off due to many reasons, including spinal misalignment issues, spinal curvature issues, osteoarthritic changes and disc bulges.
A foraminal disc bulge is one of the structures that can compress a nerve as it leaves the neuroforaminal space, potentially causing significant symptoms including pain, tingling, weakness or numbness in the area of the anatomy served by the affected nerve structure.
Foraminal Herniated Disc Concerns
Pinched nerves are diagnosed far more often than they actually occur in the spine. In many cases, the disc may well block much of the neuroforaminal space, but there is still plenty of room for the nerve to exit without suffering any compression at all. Simple contact with the nerve is not at all likely to produce symptoms. Instead, the foraminal space would need to be virtually sealed and the bulge would need to actually compress the nerve fibers to elicit a symptomatic expression.

I always suggest clinical correlation with a neurologist for any suspected nerve compression syndrome, since often, the symptoms will not match the expectations for the diagnostic theory. In fact, in most cases, the symptoms will prove far too wide ranging for a single level compressive neuropathy condition to enact.
Remember that even large herniations do not necessarily cause any pain or other related symptoms. The disc must actually affect the viability of the nerve structure in order for these symptoms to occur in the case of foraminal stenosis leading to a pinched nerve diagnosis.
Foraminal Bulging Disc Discussion
Foraminal herniations can be focal or diffuse and many are also classifiable as other types of herniations, including paramedian bulges.
Treatment options for pinched nerves are often incredibly unenlightened. Assuming that the disc is actually pinching the nerve, how can such common conservative care practices as physical therapy or drugs cure it? They can’t. They won’t. Strangely, many patients seem to do better with the passage of time alone, compared to any specific conservative care approach.
It should be noted that many patients who have been misdiagnosed and are actually suffering from ischemic back pain will typically respond well to the alternative treatment path offered by knowledge therapy.
In the case of true objective weakness or numbness and associated muscular dysfunction, the chances for an actual compressive neuropathy rise. However, this is a rule with possible exceptions. Remember to consider all possible explanations for your symptoms, particularly if they do not correlate precisely to the clinical expectations of the diagnosis.
Herniated Disc > What is a Herniated Disc > Foraminal Herniated Disc


